SHARE
Services for the Health in Asian & African Regions (SHARE) = SHARE is a citizen sector organization (NGO) that engages in international cooperation mainly through providing health service.
HOME > News > Information of COVID-19(4)
- 【※updated】COVID-19(multi-language)
- Information of COVID-19(15)
- Information of COVID-19(vaccines)
- 《Request to the Government of Japan》Ease the protection of intellectual property rights and promote sharing and cooperating on pharmaceuticals and medical technologies, in order to accelerate efforts to overcome COVID-19 all over the world.
- Information of COVID-19(14)
- Information of COVID-19(13)
- Information of COVID-19(12)
- Information of COVID-19(11)
- SHARE Medical Information Line for Migrants is resumed in Oct.
- Information of COVID-19(10)



Information of COVID-19(4)

Information of COVID-19 (4)by SHARE 2020.04.20
1.Global and Japanese Situation of COVID-19
Confirmed cases of COVID-19 worldwide according to reports by WHO Update 2020/4/12 (Japan Standard Time) : Ministry of Health, Labor and Welfare (MHLW)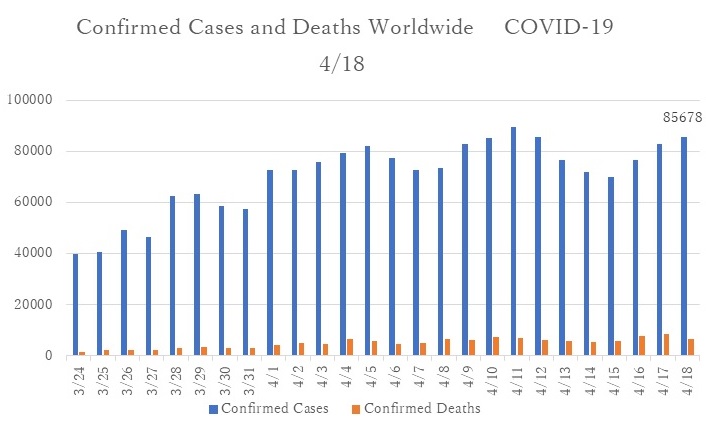
Tokyo 2020/4/18 (Japan Standard Time): Tokyo Prefecture Report
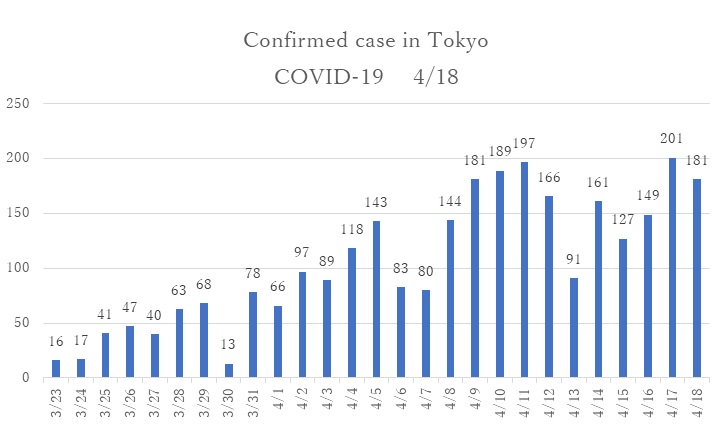
- The number of confirmed cases continues to exceed 100 cases per day after the Japanese government declared the state of emergency on 7 April.
- On April 16, the Japanese government declared the national state of emergency to prevent further spread of COVID-19 virus from high populated prefectures to other areas.
2.First「National survey on COVID-19」on 31 March to 1 April, 2020
- The joint survey was conducted collaboration of MHLW and LINE Corporation. 24 million of Japanese residents (approximately 20 percent of total population) participated in this survey. The survey was an innovative survey method that enabled to collect data in limited time with low-cost. However, because the targeted population was people who used LINE in daily life, this survey methods showed some limitations: People with severe symptoms had low respond rates due to difficulty of engaging in LINE; People with high health literacy of infection prevention more likely to present the high respond rates.
- The questionnaire consisted of age, zip-code, gender, and health condition (normal, fever more than 37.5 ℃, sore throat, strong fatigue, cough, other not feeling well).
- The participants were categorized into six groups: (1) People who were in the service industry and could not avoid the three Cs[1](e.g., food services, salespeople that involve face-to-face contacts); (2)People who obtained knowledge of the infection prevention (e.g., health professionals, long-term care specialists); (3) People who were involved in works where already implemented measures to avoid three Cs (e.g., office work, retail industry, delivery services); (4) People who were involved in schools where temporarily closed as they followed measures to avoid three Cs (e.g., teachers, school staff, and students); (5) People who were able to practice social distance (e.g., housewives); and (6) People who did not belong to any of groups mentioned above.
- The participants in Group (1) reported having a fever (more than 37.5 ℃ for four days) relatively higher than other groups (0.23% of total participants in Group (1)) in nationwide.
- The proportion of participants who reported having a fever was highest in Tokyo metropolitan(0.38%).
- Participants in Group (5) reported having the least fever. From this result, it is considered that Group (5) may have been practicing social distances and measures to avoid the three Cs. This result showed that it is useful to prevent unnecessary outings to infect yourself or spread the infection to others.
- Group (1) could be the most vulnerable people to the risk of virus infection due to the nature of their working environments. It is urgently necessary to coordinate infection prevention measures to avoid the three Cs.
- The proportion of fever among Group (2) and Group (3) may correlatively increase as the infection risk increased in the community. It is necessary to maintain working environment with the measures to avoid the three Cs and to take social distance. Essential services (medicine, long-term care, retail industry, and delivery services) may require managing standard precautions under the critical circumstances.
- Group (4) is currently maintaining a social distance with the emergency school closures. Preparation of infection prevention practices is important for the resumption of school, such as face-to-face infection prevention education to avoid the 3 Cs, utilizing ICT for distance learning, and regular health checkups.
(Result 1)
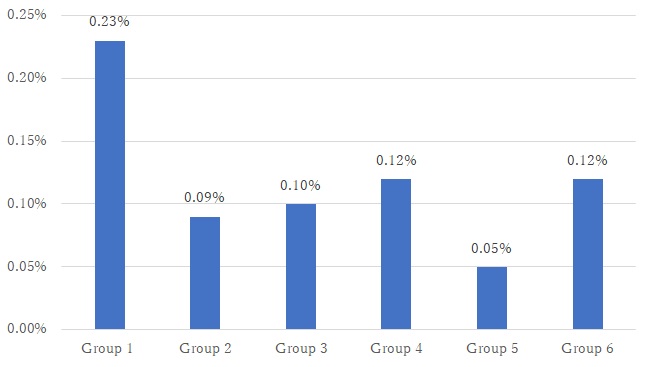
Figure 1 The proportion of participants who reported having a fever
(Result2)
(Recommendation: Required measures by the group)
Closed spaces, Close proximity to others, and Close conversation
3.Was a new coronavirus infection epidemic predicted?(Emerging infectious Disease)
- COVID-19 and Ebola virus disease are emerging infectious diseases. According to WHO, the emerging infectious disease is defined as 'Newly recognized, newly evolved or occurred previously but have shown an increase in incidence or expansion of geographical, vector or host range'. Emerging infectious diseases have been under scrutiny since the 1990s, and they have become one of the most critical public health issues in the global health community, including avian flu, SARS, and MERS.
- A PUBLIC HEALTH EMERGENCY OF INTERNATIONAL CONCERN (PHEIC) is a formal declaration by the WHO as 'an extraordinary public health event which constitutes a public health risk to other States through the international spread of disease and may require a coordinated international response'. Under the 2005 International Health Regulations, countries have a legal duty to respond promptly to a PHEIC. Such events are required to be assessed for notification to WHO using a decision instrument. Four decision criteria used in the assessment of a public health event are (a) The seriousness of the event's public health impact. (b) The unusual or unexpected nature of the event. (c) The risk of international spread. (d) The risk that other countries will impose travel or trade restrictions. Any two criteria must notify to the WHO.
- A single case of smallpox, poliomyelitis (WPV), human influenza caused by a new subtype, and SARS must be immediately reported to WHO, irrespective of the context in which it occurs.
- In global context, strategies, measures, and specific action plans have been prepared for emerging infectious diseases such as COVID-19 infections. However, the COVID-19 infection had unexpected impact due to the following reasons:
1:Typically, infectious disease spreads after patients become symptomatic. The new coronavirus has spread widely in asymptomatic cases.
2:Strategies and measures were prepared in the context of low- and middle- income countries where the health system is fragile, and to prevent pandemic to high-income countries. Explosive infections were not expected to prevail in high-income countries.
(Unexpected characteristics of COVID-19 infection)
Referenceand further information:
1.https://www.mhlw.go.jp/stf/newpage_10798.html
2.https://www.japantimes.co.jp/news/2020/04/06/national/japan-social-distancing-talking-coronavirus/#.XpwZGy2KU0o
3.https://www.who.int/docs/default-source/documents/health-topics/standard-precautions-in-health-care.pdf?sfvrsn=7c453df0_2
4.https://www.who.int/ihr/procedures/pheic/en/
Written by Nakasa T, MD, Co-President of SHARE
Koto K, RN, SHARE advisor
Koto K, RN, SHARE advisor
■English Information
-
Information of COVID-19(1)(ENGLISH)
-
Information of COVID-19(2)(ENGLISH)
-
Information of COVID-19(3)(ENGLISH)
-
Information of COVID-19(4)(ENGLISH)
-
Information of COVID-19(5)(ENGLISH)
-
Information of COVID-19(6)(ENGLISH)
-
Information of COVID-19(7)(ENGLISH)
-
Information of COVID-19(8)(ENGLISH)
-
Information of COVID-19(9)(ENGLISH)
■Useful URLs by multi-languages


- Donation/Fund-raise:The share is recognition NPO. The contribution of everybody becomes the object of the deduction.
-
-

Donate Online
-
Monthly Support Program
-

BOOK
-
post card, stamp
-
Services for the Health in Asian & African Regions (SHARE)
Maruko bldg. 5F, 1-20-6, Higashi-Ueno, Taito-ku, Tokyo, 110-0015 JAPAN
TEL 81-3-5807-7581/FAX 81-3-3837-2151![]() facebook
facebook